Recently there has been a fair bit of talk about Ovarian Cancer, however all the cysts are not cancer, there are lots of different types of cysts on the ovaries which are harmless, particularly in young women.
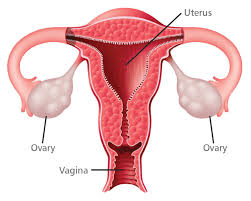
What are ovaries?, they are the main sex organs in the female who along with the uterus perform the human reproductive function. Ovaries along with their tubes are referred as Adnexa.

These amazing organs lay dormant until puberty then they become active for 30 to 40 years of a women's reproductive life and then they stop again and this is then called Menopause.
Scientists are still trying to study what suddenly brings on puberty.
I think that they are close to solving this puzzle.
Scattered in the ovary are millions of immature eggs. these are called primordial follicles.
In the foetal ovary there are millions of these , at puberty there are about four hundred thousand, they gradually mature into eggs, the rest dry up and at menopause we run out of them.
As the primordial follicle matures it makes a cyst that is a cavity full of fluid, this has hormones and this is called follicle cyst. This is one of the common cause of pelvic pain, especially in the midcycle when it is growing and releases the egg. Sometimes it overgrows and causes a follicular cyst, which causes pain. After the follicle ruptures it forms another cyst, which is called corpus luteum cyst and when picked up by ultrasound , both these cysts cause anxiety in women, however they are not cancerous. We call them physiological cysts as they are the result of cyclical ovarian function.
They are causing symptoms , such as acute pain, haemorrhage, torsion(twisted), grow bigger than five centimetres and do not resolve by themselves, then they require surgical removal which can be done by key hole surgery. It is often best not to disturb the corpus luteum cyst as it can bleed during surgery and subsequently causes scar tissue.
There are many different types of ovarian cysts and we will discuss these in another post, and most of these are often pain free, unless touched during intercourse.
The other Adnexal Pathology that causes Acute Dyspareunia is an ectopic pregnancy , which means pregnancy in the tube. The diagnosis is made by a pregnancy test and an ultrasound. Again urgent treatment is recommended.
The other ovarian conditions related to acute pain not necessarily related to dyspareunia are torsion of the ovary, rupture of an ovarian cyst. All these conditions require urgent medical attention.







