While we are talking about Dyspareunia, let us complete the subject by talking about Superficial Vaginal Infections(SVI) and inflammatory conditions called Vulvar Dermatoses, they also cause Dyspareunia, Vulvo Vaginal Pruritus and Vaginal Discharge.
All women have vaginal discharge during their reproductive life, in varying amounts during their menstrual cycle. I wonder if any of you have ever thought what a great house keeping function this discharge does by keeping the vagina clean, by washing away the dead cells and infections.
This normal vaginal discharge comes from the glands located in cervix and the vagina.
There is increased discharge at appropriate times such as ovulation and sexual arousal.
It is very important to keep the personal vaginal hygiene up to date.
The question is where do these infections come from, some of the organisms are locally present and under conditions favourable to them , they start playing around and cause disease, the commonest of these is a fungus called Candida.
On other occasions the infections come after child birth, pelvic operations, sexual intercourse, unscientific use of antiseptics, scented soaps, bubble baths and washes and the list can go on.
The main discharge problems along with pain and pruritus are as follows;
1-Candidiasis,2-Bacterial Vaginosis,3-Trichomonas,4- Nabothian Follicles,5-Cytolitic Vaginosis,6-Streptococcal Vaginosis,7-Erosive Vaginitis,8-Atrophic Vaginitis,9-Chlamydia,10-Gonococcus,11-Foreign Body, 12-Malignancy.
We have already discussed Chlamydia and Gonococcus in our previous post on PID, its difficult to discuss all the above conditions, but we will discuss the commonest of these being Candidiasis, Bacterial Vaginosis, and Trichomonas.
VULVO VAGINAL CANDIDIASIS(VVC)
It is estimated that 50 to 70 percent of women of all ages during their reproductive life suffer from at least one episode of VVC.
They generally do not suffer prepuberty and postmenopausal, because Candida loves oestrogen and oestrogen milieu and during this period of life is absent or low.
The infection is caused by a variety of Candida Albicans, the other variety of Candida often found is called Candida Glabrata and this requires special and stronger treatment.
Vulva and Vagina are both involved but often not together. In diabetic women VVC is often very severe the area looks very inflamed and swollen and the infection spreads to the groin and perianal area.
The symptoms of VVC can be mild or severe and they include severe itching, and maybe pain on passing urine. The risk factors are pregnancy when the oestrogen level is high, use of antibiotics, diabetes, and HRT.
The diagnosis is easy considering the history, and examination which shows redness and white curdy discharge in the area.
There is a simple office microscopic test using saline and sodium hydroxide which shows fine filaments which is called pseudohyphae, this test also shows Trichomonas vaginalis -this organism will be readily recognisable by its characteristic movement.
Bacterial vaginosis -have a special cell, called a clue-cells.
We can also see the hormone status of the individual by looking at the vaginal cells. So this test gives a lot of information. Still it is best to send a vaginal swab, cervical cytology and STD test in high risk patients.
The treatment of VVC is to remove the risk factors, control diabetes and for the very first episode, local vaginal nystatin cream for one week, this can be used during pregnancy as well. It is important to clear candidiasis in pregnant women because it can be passed on to the baby at birth as an oral infection, subsequently the baby can pass it on to the mother during breast feeding.
If candidiasis persists we have to look for the reasons for persistence, I often do a glucose tolerance test to exclude diabetes, if they are on high dosage oestrogen pill, change the pill or use a different type of contraception. Depoprovera and Mirena are good alternatives. Mirena is a progesterone releasing intrauterine device. DPMA is an injectable progestron which is given by a IM injection of 150mg every three months.
Both these are good long term contraceptives and help in getting rid of chronic candidiasis.
Long term recurrence requires long term treatment, which is given over a period of six months.
1- Vaginal nystatin pessaries every night or alternate night for six months.
2-Oral flucanazole of 100mg twice weekly for six months.
3-Oral ketoconazole 200mg a day for six months. This is hepatoxic, so the liver needs to be tested every two to three months.
The vagina can be painted with gentian violet weekly for several weeks.
Once again the subject that we have just discussed needs more time and information and this will be followed up in our next post.
Monday, September 16, 2013
Monday, August 12, 2013
PELVIC INFLAMMATORY DISEASE
Michelle aged 33 came to see me complaining of infertility, meaning that she was unable to conceive within the last fourteen months, she was advised that the reason for this is damage to her tubes.
She was not aware of any illnesses that may have caused this, my immediate reaction was that she probably had very mild pelvic inflammatory disease at college, which often can be silent and can cause tubal damage.
Technically (PID) is a term used to express infection of the uterus , tubes and ovaries, which often results in long term damage of the tubes, adhesions and infertility. This causes chronic Dyspareunia, pelvic pain and backache.
I feel that the infections of the cervix, vagina and vulva should also be included as PID.
The main reason for PID in younger people is by sexually transmitted infections, the typical person having these problems is a young women having periods and sexually active.
The other causes of PID are infections during an abortion or miscarriage, intrauterine devices and blood born diseases, such as Tuberculosis which is relatively rare in the western world.
The infecting organisms, Chlamydia Trachomatis, Neisseria Gonorrhoea are sexually transmitted bacteria which can cause asymptomatic infection or very serious disease.
Other sexually transmitted disease are Herpes Virus, which causes changes in the cervix called cervical dysplasia and this if progressed can lead to cervical cancer, this does not cause an infection of the uterus, tubes or the ovaries or in other words the internal organs. Trichomonas Vaginalis which is not a bacteria but is a protozoa. (A type of infecting organism) which is also sexually transmitted. It mainly affects the vagina causing smelly discharge and itching.
Other organisms that live happily in that region are likely to cause infection such as streptococcus Ecoli.
The diagnosis in Michelle's case was made by laparoscopy when on testing the tubes they were found to be blocked and convoluted. This can also be tested by a radiological test , but laparoscopy gives better information as regards adhesions in the pelvis. So obviously she must have had a silent episode of PID in her younger years. By the frequent nature of silent STD's amongst young women it was assumed that this was also an STD. A cervical swab was performed for Chlamydia and Gonorrhoea but as expected it was negative for both. Besides the swabs, laparoscopy and ultrasound often prior to laparoscopy and blood tests are also performed. The blood test which can give us an idea of an active infection is called CRP.
When you have mild symptoms of pelvic pain, altered menstrual function, pain on intercourse, please do not ignore them and do not run the risk of silent PID, as we have learnt in Michelle's case the long term consequences can be permanent.
Thanks to modern assisted reproductive technology, Michelle was helped to have a healthy baby.
When a women presents with pelvic pain, altered bleeding, there are many other conditions that have to be kept in mind. One of the most important is an Ectopic Pregnancy. The current pregnancy tests are extremely accurate, and if it is a positive result it's highly possible that the women has an Ectopic Pregnancy , this could be the result of a past or present PID.
Other diagnoses that should be remembered are appendicitis, septic abortion, haemorrhagic ruptured ovarian cyst, twisted ovary, degenerating fibroid and enteritis.
Clinical history, pelvic examination, blood test, pregnancy test, ultrasound, swab test, and finally laparoscopy will give us the diagnosis.
The treatment depends on the cause and in PID multiple antibiotic therapy is recommended as often we are unable to grow the infecting organism in PID.
It is very important to clear the PID as the long term consequences are serious and dangerous, as already mentioned it can cause infertility, chronic PID, chronic adhesions even affecting the liver, Ectopic Pregnancy, and even death in some situations.
PID is a serious disease and every attempt should be made to treat it early on very minor symptoms, such as vaginal discharge, pain and bleeding.
The most important thing is to have regular medical check ups if you are sexually active, and should you have a new sexual partner have him tested for STD's.
The second thing is do not take over the counter medicines for vaginal discharge or itch, without a proper diagnosis. All that itches is not thrush.
I have seen a women in her seventies who was treating herself for thrush and in fact it was vulval carcinoma.
Post menopausal women do not get thrush unless they are diabetic or taking excessive HRT.
Although women who are post menopausal, are not so prone to PID, but occasionally they get a collection of pus inside the uterus called pyometra, this needs treatment.
The moral of the story is do not consider vaginal discharge insignificant, have it seen to, and do not treat yourself.
We will discuss the superficial pelvic infections on my next post.
She was not aware of any illnesses that may have caused this, my immediate reaction was that she probably had very mild pelvic inflammatory disease at college, which often can be silent and can cause tubal damage.
Technically (PID) is a term used to express infection of the uterus , tubes and ovaries, which often results in long term damage of the tubes, adhesions and infertility. This causes chronic Dyspareunia, pelvic pain and backache.
I feel that the infections of the cervix, vagina and vulva should also be included as PID.
The main reason for PID in younger people is by sexually transmitted infections, the typical person having these problems is a young women having periods and sexually active.
The other causes of PID are infections during an abortion or miscarriage, intrauterine devices and blood born diseases, such as Tuberculosis which is relatively rare in the western world.
The infecting organisms, Chlamydia Trachomatis, Neisseria Gonorrhoea are sexually transmitted bacteria which can cause asymptomatic infection or very serious disease.
Other sexually transmitted disease are Herpes Virus, which causes changes in the cervix called cervical dysplasia and this if progressed can lead to cervical cancer, this does not cause an infection of the uterus, tubes or the ovaries or in other words the internal organs. Trichomonas Vaginalis which is not a bacteria but is a protozoa. (A type of infecting organism) which is also sexually transmitted. It mainly affects the vagina causing smelly discharge and itching.
Other organisms that live happily in that region are likely to cause infection such as streptococcus Ecoli.
The diagnosis in Michelle's case was made by laparoscopy when on testing the tubes they were found to be blocked and convoluted. This can also be tested by a radiological test , but laparoscopy gives better information as regards adhesions in the pelvis. So obviously she must have had a silent episode of PID in her younger years. By the frequent nature of silent STD's amongst young women it was assumed that this was also an STD. A cervical swab was performed for Chlamydia and Gonorrhoea but as expected it was negative for both. Besides the swabs, laparoscopy and ultrasound often prior to laparoscopy and blood tests are also performed. The blood test which can give us an idea of an active infection is called CRP.
When you have mild symptoms of pelvic pain, altered menstrual function, pain on intercourse, please do not ignore them and do not run the risk of silent PID, as we have learnt in Michelle's case the long term consequences can be permanent.
Thanks to modern assisted reproductive technology, Michelle was helped to have a healthy baby.
When a women presents with pelvic pain, altered bleeding, there are many other conditions that have to be kept in mind. One of the most important is an Ectopic Pregnancy. The current pregnancy tests are extremely accurate, and if it is a positive result it's highly possible that the women has an Ectopic Pregnancy , this could be the result of a past or present PID.
Other diagnoses that should be remembered are appendicitis, septic abortion, haemorrhagic ruptured ovarian cyst, twisted ovary, degenerating fibroid and enteritis.
Clinical history, pelvic examination, blood test, pregnancy test, ultrasound, swab test, and finally laparoscopy will give us the diagnosis.
The treatment depends on the cause and in PID multiple antibiotic therapy is recommended as often we are unable to grow the infecting organism in PID.
It is very important to clear the PID as the long term consequences are serious and dangerous, as already mentioned it can cause infertility, chronic PID, chronic adhesions even affecting the liver, Ectopic Pregnancy, and even death in some situations.
PID is a serious disease and every attempt should be made to treat it early on very minor symptoms, such as vaginal discharge, pain and bleeding.
The most important thing is to have regular medical check ups if you are sexually active, and should you have a new sexual partner have him tested for STD's.
The second thing is do not take over the counter medicines for vaginal discharge or itch, without a proper diagnosis. All that itches is not thrush.
I have seen a women in her seventies who was treating herself for thrush and in fact it was vulval carcinoma.
Post menopausal women do not get thrush unless they are diabetic or taking excessive HRT.
Although women who are post menopausal, are not so prone to PID, but occasionally they get a collection of pus inside the uterus called pyometra, this needs treatment.
The moral of the story is do not consider vaginal discharge insignificant, have it seen to, and do not treat yourself.
We will discuss the superficial pelvic infections on my next post.
Monday, July 22, 2013
RESIDUAL OVARY OR OVARIAN REMENANT SYNDROME
Stephanie aged 48, came to see me with severe Dyspareunia.
She had a Hysterectomy with the ovaries conserved six years ago, and for the last two years this pain was gradually increasing, she had seen two other clinicians who had advised her to use local oestrogen cream and maybe change coital position. This treatment did not help her.
When I saw her on examination her vagina was not dry and she was tender on both sides where her ovaries were supposed to be located, and on moving the vaginal apex she felt pain.
My diagnosis was immediately clear that it was what we call Residual Ovary Syndrome(ROS).
A pelvic ultrasound was performed , this did not show any disease of the ovaries. I offered Stephanie Bilateral Salpingo-oophorectomy.(Removal of both tubes and ovaries), followed by hormone replacement.
Stephanie agreed to this and was a million dollars after treatment.
ROS is a condition which is not often thought of and many times women are older and are reluctant to discuss the condition of dyspareunia. Even if they do, they are more often offered local treatment.
ROS has been found to happen in two to three percent of cases after hysterectomy when the ovaries have been conserved. Usually three percent of these are found to be cancerous. Arguments continue if the ovaries should be removed with each hysterectomy. The general consensus of opinion is that if a woman is older than 45, removal should be considered depending on the woman's risk factors if she takes HRT for a long time. These are family history of breast cancer, stroke, deep venous thrombosis and heart disease.
If there is a family history of ovarian cancer it can become a bit tricky.
The final decision should be made by the woman depending on her individual choice.
ROS is characterised by pelvic pain, pelvic mass and dyspareunia. When a woman presents with one or more of these symptoms a clinical examination should be performed. An ultrasound examination often gives a diagnosis if there is an ovarian cyst or a mass. Further evaluation can give an idea if there is any suggestion of malignancy. Often a CT and a MRI is performed which can help the diagnosis in difficult cases. Sometimes these cysts arise from the peritoneum, which is a membrane that covers the inside of our belly.
The blood test for the patients general health and hormone studies to assess the ovarian function are useful. There is a test called CA125 which is a screening test for cancer, if it shows a low value, we can assume that there is no cancer.
If we have excluded ovarian cancer with certainty by our tests, then the treatment can be one of the following;
1- Can be medical by hormones-Depo-Provera, GnRH Analogues, both these hormones suppress the ovaries and give temporary relief.
2- Aspiration of the cyst on the ovary, this fluid is sent for testing to exclude any cancer cells. This is also temporary, but it can be repeated more than once.
3- Radiation of the ovaries will stop them making physiological cysts.
4- The final and definitive treatment is by the removal of the ovaries or the remnants. This can be done either by key hole surgery or open surgery. This can be a difficult surgery because the adhesion's form around the ovaries, involving the bowel and ureter which can be damaged in the process.
In the first place these remnants are left behind because the initial operation was difficult due to pelvic adhesion's as a result of endometriosis and pelvic infections.
This has to be followed by supervised hormone replacement.
5 If there is any doubt about the ovarian mass or cyst being cancerous have it removed.
In summarising do not ignore post hysterectomy pelvic pain if you have one or both of your ovaries, have the necessary investigations and treatment. Do not be frightened of Hormone Replacement Treatment, it can make your life very comfortable if given under proper supervision.

She had a Hysterectomy with the ovaries conserved six years ago, and for the last two years this pain was gradually increasing, she had seen two other clinicians who had advised her to use local oestrogen cream and maybe change coital position. This treatment did not help her.
When I saw her on examination her vagina was not dry and she was tender on both sides where her ovaries were supposed to be located, and on moving the vaginal apex she felt pain.
My diagnosis was immediately clear that it was what we call Residual Ovary Syndrome(ROS).
A pelvic ultrasound was performed , this did not show any disease of the ovaries. I offered Stephanie Bilateral Salpingo-oophorectomy.(Removal of both tubes and ovaries), followed by hormone replacement.
Stephanie agreed to this and was a million dollars after treatment.
ROS is a condition which is not often thought of and many times women are older and are reluctant to discuss the condition of dyspareunia. Even if they do, they are more often offered local treatment.
ROS has been found to happen in two to three percent of cases after hysterectomy when the ovaries have been conserved. Usually three percent of these are found to be cancerous. Arguments continue if the ovaries should be removed with each hysterectomy. The general consensus of opinion is that if a woman is older than 45, removal should be considered depending on the woman's risk factors if she takes HRT for a long time. These are family history of breast cancer, stroke, deep venous thrombosis and heart disease.
If there is a family history of ovarian cancer it can become a bit tricky.
The final decision should be made by the woman depending on her individual choice.
ROS is characterised by pelvic pain, pelvic mass and dyspareunia. When a woman presents with one or more of these symptoms a clinical examination should be performed. An ultrasound examination often gives a diagnosis if there is an ovarian cyst or a mass. Further evaluation can give an idea if there is any suggestion of malignancy. Often a CT and a MRI is performed which can help the diagnosis in difficult cases. Sometimes these cysts arise from the peritoneum, which is a membrane that covers the inside of our belly.
The blood test for the patients general health and hormone studies to assess the ovarian function are useful. There is a test called CA125 which is a screening test for cancer, if it shows a low value, we can assume that there is no cancer.
If we have excluded ovarian cancer with certainty by our tests, then the treatment can be one of the following;
1- Can be medical by hormones-Depo-Provera, GnRH Analogues, both these hormones suppress the ovaries and give temporary relief.
2- Aspiration of the cyst on the ovary, this fluid is sent for testing to exclude any cancer cells. This is also temporary, but it can be repeated more than once.
3- Radiation of the ovaries will stop them making physiological cysts.
4- The final and definitive treatment is by the removal of the ovaries or the remnants. This can be done either by key hole surgery or open surgery. This can be a difficult surgery because the adhesion's form around the ovaries, involving the bowel and ureter which can be damaged in the process.
In the first place these remnants are left behind because the initial operation was difficult due to pelvic adhesion's as a result of endometriosis and pelvic infections.
This has to be followed by supervised hormone replacement.
5 If there is any doubt about the ovarian mass or cyst being cancerous have it removed.
In summarising do not ignore post hysterectomy pelvic pain if you have one or both of your ovaries, have the necessary investigations and treatment. Do not be frightened of Hormone Replacement Treatment, it can make your life very comfortable if given under proper supervision.

Monday, July 15, 2013
ADNEXAL CAUSES OF DYSPAREUNIA
Mary went to see her Gynaecologist all upset to find that she had a cyst on the left ovary.
Recently there has been a fair bit of talk about Ovarian Cancer, however all the cysts are not cancer, there are lots of different types of cysts on the ovaries which are harmless, particularly in young women.
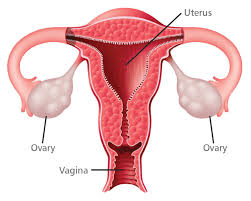
What are ovaries?, they are the main sex organs in the female who along with the uterus perform the human reproductive function. Ovaries along with their tubes are referred as Adnexa.
 The above diagram shows the maturation of the egg.
The above diagram shows the maturation of the egg.
These amazing organs lay dormant until puberty then they become active for 30 to 40 years of a women's reproductive life and then they stop again and this is then called Menopause.
Scientists are still trying to study what suddenly brings on puberty.
I think that they are close to solving this puzzle.
Scattered in the ovary are millions of immature eggs. these are called primordial follicles.
In the foetal ovary there are millions of these , at puberty there are about four hundred thousand, they gradually mature into eggs, the rest dry up and at menopause we run out of them.
As the primordial follicle matures it makes a cyst that is a cavity full of fluid, this has hormones and this is called follicle cyst. This is one of the common cause of pelvic pain, especially in the midcycle when it is growing and releases the egg. Sometimes it overgrows and causes a follicular cyst, which causes pain. After the follicle ruptures it forms another cyst, which is called corpus luteum cyst and when picked up by ultrasound , both these cysts cause anxiety in women, however they are not cancerous. We call them physiological cysts as they are the result of cyclical ovarian function.
They are causing symptoms , such as acute pain, haemorrhage, torsion(twisted), grow bigger than five centimetres and do not resolve by themselves, then they require surgical removal which can be done by key hole surgery. It is often best not to disturb the corpus luteum cyst as it can bleed during surgery and subsequently causes scar tissue.
There are many different types of ovarian cysts and we will discuss these in another post, and most of these are often pain free, unless touched during intercourse.
The other Adnexal Pathology that causes Acute Dyspareunia is an ectopic pregnancy , which means pregnancy in the tube. The diagnosis is made by a pregnancy test and an ultrasound. Again urgent treatment is recommended.
The other ovarian conditions related to acute pain not necessarily related to dyspareunia are torsion of the ovary, rupture of an ovarian cyst. All these conditions require urgent medical attention.
Recently there has been a fair bit of talk about Ovarian Cancer, however all the cysts are not cancer, there are lots of different types of cysts on the ovaries which are harmless, particularly in young women.
What are ovaries?, they are the main sex organs in the female who along with the uterus perform the human reproductive function. Ovaries along with their tubes are referred as Adnexa.
These amazing organs lay dormant until puberty then they become active for 30 to 40 years of a women's reproductive life and then they stop again and this is then called Menopause.
Scientists are still trying to study what suddenly brings on puberty.
I think that they are close to solving this puzzle.
Scattered in the ovary are millions of immature eggs. these are called primordial follicles.
In the foetal ovary there are millions of these , at puberty there are about four hundred thousand, they gradually mature into eggs, the rest dry up and at menopause we run out of them.
As the primordial follicle matures it makes a cyst that is a cavity full of fluid, this has hormones and this is called follicle cyst. This is one of the common cause of pelvic pain, especially in the midcycle when it is growing and releases the egg. Sometimes it overgrows and causes a follicular cyst, which causes pain. After the follicle ruptures it forms another cyst, which is called corpus luteum cyst and when picked up by ultrasound , both these cysts cause anxiety in women, however they are not cancerous. We call them physiological cysts as they are the result of cyclical ovarian function.
They are causing symptoms , such as acute pain, haemorrhage, torsion(twisted), grow bigger than five centimetres and do not resolve by themselves, then they require surgical removal which can be done by key hole surgery. It is often best not to disturb the corpus luteum cyst as it can bleed during surgery and subsequently causes scar tissue.
There are many different types of ovarian cysts and we will discuss these in another post, and most of these are often pain free, unless touched during intercourse.
The other Adnexal Pathology that causes Acute Dyspareunia is an ectopic pregnancy , which means pregnancy in the tube. The diagnosis is made by a pregnancy test and an ultrasound. Again urgent treatment is recommended.
The other ovarian conditions related to acute pain not necessarily related to dyspareunia are torsion of the ovary, rupture of an ovarian cyst. All these conditions require urgent medical attention.
Wednesday, July 3, 2013
PELVIC CONGESTION SYNDROME
In our previous posts we enumerated some causes of Deep Dyspareunia and we are endeavouring to cover all these causes, in a little bit more detail but not in the order that we posted previously.
In this post we will focus on Pelvic Congestion Syndrome (PCS). Nearly 30 percent of women suffer from this condition in their lifetime. The top age group is between 20 to 45 years of age. It is caused by , varicose veins in the pelvis around the uterus and ovaries, similar to varicose veins in the legs.
It is not understood if there is a genetic factor or anatomical factor in the formation of the veins.
The women suffer from chronic lower abdominal discomfort, backache and pain on intercourse, it gets worse at the end of the day and after sex.
The other symptoms they suffer is heavy painful periods, vaginal discharge, bladder discomfort and mood swings.
It usually happens after child birth, with the hormone changes and weight gain during pregnancy, which puts pressure on the ovarian veins and the blood flow is impeded. High levels of oestrogen during pregnancy dilates the veins, further contributing to the problem. With each pregnancy over time the uterus enlarges, the lining of the uterus becomes thicker and often the uterus falls backwards(this is called Retroversion), this further adds to the problem of dyspareunia, the periods become heavier and painful.
The diagnosis of PCS is difficult because there are nearly twenty other conditions which cause the complex chronic backache, heavy and painful periods and dyspareunia.
About twenty years ago we offered them medical treatment, often followed by hysterectomy.This did not really help the women and their symptoms continued. The removal of the ovaries was more helpful, but then the problem was of sudden surgical menopause and hormone replacement was required. And we replaced one problem with another.
Luckily we have learnt a lot more about PCS and are able to help the vast majority of women.
Most of the clinicians being aware of the problem, try to tackle it in the modern way.
The history and clinical examination helps us to exclude many other conditions, such as large fibroids and ovarian cysts.
The diagnosis is of exclusion of other causes. An ultrasound examination is useful to exclude other pathology, but often it does not highlight the veins because it is carried out in a supine position. The new colour ultrasound is useful if available to show us the uterine congestion.
CT and MRI is useful however CT is more invasive as we have to use injection of dyes to highlight the problem and the patient is exposed to radiation.
Venogram is most helpful in making a diagnosis, as it is not too drastic. Only, it has to be done by a special radiologist at a specialist centre.
They can inject the veins with sclerosing agents to block them and they can put little clips inside the veins so that the backward blood flow is stopped. This simple treatment of embolization gives women satisfactory results for several years. The very latest diagnostic and therapeutic technology to manage this condition, treating it effectively with a minimally invasive outpatient procedure.


 These pictures show the vascular uterus on colour ultrasound, a venogram of pelvic organs with venous congestion, and post treatment ,left ovarian vein.
These pictures show the vascular uterus on colour ultrasound, a venogram of pelvic organs with venous congestion, and post treatment ,left ovarian vein.
For those women who cannot avail themselves of the most current and remarkable treatment for PCS
the old medical treatment still helps.
This consists of pain relief by non steroidal antinflammatory medications, oral contraceptive pills, and drugs to suppress the ovaries. Some people believe in Acupuncture, Homeopathic and Osteopathy. Surely all this can be tried with adequate rest and counselling.
In the next post we will talk about Adnexal Pathology (Tubes and Ovaries)
In this post we will focus on Pelvic Congestion Syndrome (PCS). Nearly 30 percent of women suffer from this condition in their lifetime. The top age group is between 20 to 45 years of age. It is caused by , varicose veins in the pelvis around the uterus and ovaries, similar to varicose veins in the legs.
It is not understood if there is a genetic factor or anatomical factor in the formation of the veins.
The women suffer from chronic lower abdominal discomfort, backache and pain on intercourse, it gets worse at the end of the day and after sex.
The other symptoms they suffer is heavy painful periods, vaginal discharge, bladder discomfort and mood swings.
It usually happens after child birth, with the hormone changes and weight gain during pregnancy, which puts pressure on the ovarian veins and the blood flow is impeded. High levels of oestrogen during pregnancy dilates the veins, further contributing to the problem. With each pregnancy over time the uterus enlarges, the lining of the uterus becomes thicker and often the uterus falls backwards(this is called Retroversion), this further adds to the problem of dyspareunia, the periods become heavier and painful.
The diagnosis of PCS is difficult because there are nearly twenty other conditions which cause the complex chronic backache, heavy and painful periods and dyspareunia.
About twenty years ago we offered them medical treatment, often followed by hysterectomy.This did not really help the women and their symptoms continued. The removal of the ovaries was more helpful, but then the problem was of sudden surgical menopause and hormone replacement was required. And we replaced one problem with another.
Luckily we have learnt a lot more about PCS and are able to help the vast majority of women.
Most of the clinicians being aware of the problem, try to tackle it in the modern way.
The history and clinical examination helps us to exclude many other conditions, such as large fibroids and ovarian cysts.
The diagnosis is of exclusion of other causes. An ultrasound examination is useful to exclude other pathology, but often it does not highlight the veins because it is carried out in a supine position. The new colour ultrasound is useful if available to show us the uterine congestion.
CT and MRI is useful however CT is more invasive as we have to use injection of dyes to highlight the problem and the patient is exposed to radiation.
Venogram is most helpful in making a diagnosis, as it is not too drastic. Only, it has to be done by a special radiologist at a specialist centre.
They can inject the veins with sclerosing agents to block them and they can put little clips inside the veins so that the backward blood flow is stopped. This simple treatment of embolization gives women satisfactory results for several years. The very latest diagnostic and therapeutic technology to manage this condition, treating it effectively with a minimally invasive outpatient procedure.

For those women who cannot avail themselves of the most current and remarkable treatment for PCS
the old medical treatment still helps.
This consists of pain relief by non steroidal antinflammatory medications, oral contraceptive pills, and drugs to suppress the ovaries. Some people believe in Acupuncture, Homeopathic and Osteopathy. Surely all this can be tried with adequate rest and counselling.
In the next post we will talk about Adnexal Pathology (Tubes and Ovaries)
Monday, June 24, 2013
DEEP DYSPAREUNIA
In our previous posts we have been talking about Dyspareunia as apposed to the superficial pain of the vulva, Deep Dyspareunia is caused by deep penetration of the penis into the pelvis.
Deep Dyspareunia is usually due to pelvic pathology and the following conditions are commonly encountered.
1 Endometriosis
2 Adenomyosis
3 Acute and Chronic Pelvic Infections
4 Pelvic Congestion Syndrome
5 Adnexal Pathology
6 Retroverted Uterus
7 Residual Ovary Syndrome
8 Interstitial Cystitis
9 Dry Atrophic Tissues
10 Psychosocial Problems
Endometriosis is a condition, the cause of which we do not understand. In spite of lots of research.
In this condition the lining of the uterus can survive outside the uterus, and with each menstrual cycle has some bleed, as a result of that , some scar tissue forms. Often the blood collects and forms cysts of varying sizes. This can happen at any age group. The main symptom is painful periods, abdominal discomfort, pain on defecation and deep dyspareunia. We talked about clinical history in examination in previous posts but if you are looking for the cause of deep dyspareunia it is important to have an ultrasound and an MRI, so that diagnosis of some of the other conditions can be made.
Endometriosis also causes infertility, the definitive diagnosis is established by a surgical procedure called Laparoscopy, which in simple words mean Key Hole surgery of peeping in the belly.When Endometrios is minor it appears as dark spots which can be lasered or diathermy and this gives relief to the patient. This should be followed by oral contraception, so that the periods are small or none. With this treatment, the chances of endometriosis recurring are minimised. This often helps the women to get pregnant if they were having difficulty.

 Diathermy of Endometriotic Implants
Diathermy of Endometriotic Implants
during Laparoscopy.
Endometriosis grows under the influence of hormone oestrogen, therefore it grows during reproductive years. It eases off during pregnancy and after menopause. It is a painful condition, the main treatment needs to suppress oestrogens which can be done by many drugs, the simplest being Progesterone and continuous oral contraceptive pill.
The other part of the treatment is pain relief, and this can be done by non steroidal antinflammatory drugs.
If the endometriosis is advanced and has made large cysts , they have to be surgically removed, either by key hole surgery or open surgery. The largest endometriosis I have removed were about the size of two cantaloupes , one on each ovary.
For what ever reason this patient had no pain. The diagnosis was made by Ultrasound.
The youngest patient of endometriosis I have treated with laparoscopic diathermy was thirteen years of age. I was a bit reluctant to do this , but her mother assured me that her pain was very severe and I had to do something.
Endometriosis in itself is a very large topic and needs an individual post which I will do at a later date. But for now, you can remember that this is one of the main causes of Deep Dyspareunia.
Adenomyosis is similar to Endometriosis and here the endometrial implants are within the muscle of the uterus. Month after month there is small bleeding within the muscles of the uterus, as a result the uterus enlarges in size and the patient has heavy and painful periods. She feels as if there is a lump in her belly. When the uterus becomes enlarged it falls backwards, what is called retroverted uterus. This cause chronic pelvic pain and deep dyspareunia. This can also cause pelvic congestion adding to the symptoms. Adenomyosis until recent times was ignored as there were no definitive diagnostic criteria. Recently with the help of colour ultrasound and MRI it has become easy.
There is no definite cure for adenomyosis but we suppress the oestrogens with the pill, intrauterine device called Mirena. The cure is hysterectomy in older women, who do not desire any children and a definitive diagnosis is made when the uterus is in your hand.
 The remaining causes of Deep Dyspareunia will be covered in forthcoming posts.
The remaining causes of Deep Dyspareunia will be covered in forthcoming posts.
Deep Dyspareunia is usually due to pelvic pathology and the following conditions are commonly encountered.
1 Endometriosis
2 Adenomyosis
3 Acute and Chronic Pelvic Infections
4 Pelvic Congestion Syndrome
5 Adnexal Pathology
6 Retroverted Uterus
7 Residual Ovary Syndrome
8 Interstitial Cystitis
9 Dry Atrophic Tissues
10 Psychosocial Problems
Endometriosis is a condition, the cause of which we do not understand. In spite of lots of research.
In this condition the lining of the uterus can survive outside the uterus, and with each menstrual cycle has some bleed, as a result of that , some scar tissue forms. Often the blood collects and forms cysts of varying sizes. This can happen at any age group. The main symptom is painful periods, abdominal discomfort, pain on defecation and deep dyspareunia. We talked about clinical history in examination in previous posts but if you are looking for the cause of deep dyspareunia it is important to have an ultrasound and an MRI, so that diagnosis of some of the other conditions can be made.
Endometriosis also causes infertility, the definitive diagnosis is established by a surgical procedure called Laparoscopy, which in simple words mean Key Hole surgery of peeping in the belly.When Endometrios is minor it appears as dark spots which can be lasered or diathermy and this gives relief to the patient. This should be followed by oral contraception, so that the periods are small or none. With this treatment, the chances of endometriosis recurring are minimised. This often helps the women to get pregnant if they were having difficulty.
during Laparoscopy.
Endometriosis grows under the influence of hormone oestrogen, therefore it grows during reproductive years. It eases off during pregnancy and after menopause. It is a painful condition, the main treatment needs to suppress oestrogens which can be done by many drugs, the simplest being Progesterone and continuous oral contraceptive pill.
The other part of the treatment is pain relief, and this can be done by non steroidal antinflammatory drugs.
If the endometriosis is advanced and has made large cysts , they have to be surgically removed, either by key hole surgery or open surgery. The largest endometriosis I have removed were about the size of two cantaloupes , one on each ovary.
For what ever reason this patient had no pain. The diagnosis was made by Ultrasound.
The youngest patient of endometriosis I have treated with laparoscopic diathermy was thirteen years of age. I was a bit reluctant to do this , but her mother assured me that her pain was very severe and I had to do something.
Endometriosis in itself is a very large topic and needs an individual post which I will do at a later date. But for now, you can remember that this is one of the main causes of Deep Dyspareunia.
Adenomyosis is similar to Endometriosis and here the endometrial implants are within the muscle of the uterus. Month after month there is small bleeding within the muscles of the uterus, as a result the uterus enlarges in size and the patient has heavy and painful periods. She feels as if there is a lump in her belly. When the uterus becomes enlarged it falls backwards, what is called retroverted uterus. This cause chronic pelvic pain and deep dyspareunia. This can also cause pelvic congestion adding to the symptoms. Adenomyosis until recent times was ignored as there were no definitive diagnostic criteria. Recently with the help of colour ultrasound and MRI it has become easy.
There is no definite cure for adenomyosis but we suppress the oestrogens with the pill, intrauterine device called Mirena. The cure is hysterectomy in older women, who do not desire any children and a definitive diagnosis is made when the uterus is in your hand.
Monday, June 10, 2013
VULVODYNIA
In my previous blog we talked about Rena's story when her honeymoon became a disaster.
We talked about the reasons and their management.
Today we have a similar story about Ashley, due to another cause of Vulval pain.
This is called Vulvodynia. She has been having this painful condition for almost a year, her social and marital life is very strained and stressed and she is already seeing two clinicians without any satisfactory resolution.
Vulvodynia was described for the first time in 1880. It was already mentioned in my previous post as Super Sensitivity of the Vulva. However it was ignored almost for a hundred years, then in 1975 International Society of Vulvo Vaginal Diseases, called it Burning Vulval Syndrome.
It is a very poorly recognised female pain disorder although one in four women suffer it sometime during their lifespan from adolescence to post menopause.
The current definition of Vulvodynia by ISSVD is:
"Chronic Vulval discomfort, most often described as burning pain, occurring in the Absence of relevant visible findings or a specific, clinically identifiable, neurological disorder"
We do not yet understand the full story of Vulvodynia.
Misdiagnosis is the commonest cause of suffering, when only one point four percent seeking medical advise are correctly diagnosed. It affects the quality of life , the women get confused, there is delay in treatment and they self medicate.
Vulvodynia can be generalised , that means that it is all over the vulva, or it can be localised, the most common sites are the vestibule and the clitoral area.
 And then it is called Vulvo Vestibulitis or Clitoral Vestibulitis.
And then it is called Vulvo Vestibulitis or Clitoral Vestibulitis.
When a patient comes to you with vulval pain , you take a detailed history, of how long she has had the pain,and the events that started the pain.
Sexual activity can it be continued and Psycho Sexual relationships with her partner. It is also worthwhile to know if she has had any operation in that area, and has she had a child.
The hygiene practices are also important to know.
On examination , we should inspect the vulva, look for any ulcers, scarring and muscle spasms, called vaginismus.
We take swabs, skin scrapings, and cervical cytology to exclude any other diseases.
One of the very simple tests is to give a cotton wool swab to the patient and ask them to show where the pain is most.
The three criteria for the diagnosis of vulvodynia , is very mild pain on touch, no positive findings and mild redness of the vulva. There are very little minor glands in the vestibule that get inflamed and cause pain.
The vulvodynia can be classified into three categories : One is the intercourse despite being painful that can be carried out with some degree of discomfort. Second Category has to be discontinued due to pain and the Third is sex cannot happen.
Vulvodynia was primarily thought to be psycho sexual but we think that there is neural problems, these most often resolve in time.
Treat any existing problems that you may have come across during your investigation.
The explanation of the condition given to the patient and the reassurance that about seventy five percent can be treated helps them.
The general advice should emphasis is that they should not self medicate and get a clear cut diagnosis.
They can wash themselves with a freshly prepared saline solution consisting of two teaspoons of salt in a litre of water. They can use cold packs to relieve the pain, do not use commercial perfumes or antiseptics and wear light clothing. Try and improve your relationships and relieve the stress.
Follow the treatment for vaginismus , you may need help of a physiotherapist who is happy to give you bio feed back treatment. Electromagnetic treatment has been tried.
Neurological Antidepressants such as Amitriptyline with a small starting dose of 10mgs. It is thought to act as nerve membrane stabiliser.
Local lubricants (water based) are useful, oestrogen cream is useful in peri menopausal women.
Five percent Xylocaine cream can be applied at the time of intercourse.
Surgically vestibulectomy has been tried with significant improvement.
Now because we think that there is a neurological involvement we are doing more studies on the refining the diagnostic criteria and treatment of this very elusive condition.
The various other Vulvo Vaginal problems will be discussed in future posts.
We talked about the reasons and their management.
Today we have a similar story about Ashley, due to another cause of Vulval pain.
This is called Vulvodynia. She has been having this painful condition for almost a year, her social and marital life is very strained and stressed and she is already seeing two clinicians without any satisfactory resolution.
Vulvodynia was described for the first time in 1880. It was already mentioned in my previous post as Super Sensitivity of the Vulva. However it was ignored almost for a hundred years, then in 1975 International Society of Vulvo Vaginal Diseases, called it Burning Vulval Syndrome.
It is a very poorly recognised female pain disorder although one in four women suffer it sometime during their lifespan from adolescence to post menopause.
The current definition of Vulvodynia by ISSVD is:
"Chronic Vulval discomfort, most often described as burning pain, occurring in the Absence of relevant visible findings or a specific, clinically identifiable, neurological disorder"
We do not yet understand the full story of Vulvodynia.
Misdiagnosis is the commonest cause of suffering, when only one point four percent seeking medical advise are correctly diagnosed. It affects the quality of life , the women get confused, there is delay in treatment and they self medicate.
Vulvodynia can be generalised , that means that it is all over the vulva, or it can be localised, the most common sites are the vestibule and the clitoral area.
When a patient comes to you with vulval pain , you take a detailed history, of how long she has had the pain,and the events that started the pain.
Sexual activity can it be continued and Psycho Sexual relationships with her partner. It is also worthwhile to know if she has had any operation in that area, and has she had a child.
The hygiene practices are also important to know.
On examination , we should inspect the vulva, look for any ulcers, scarring and muscle spasms, called vaginismus.
We take swabs, skin scrapings, and cervical cytology to exclude any other diseases.
One of the very simple tests is to give a cotton wool swab to the patient and ask them to show where the pain is most.
The three criteria for the diagnosis of vulvodynia , is very mild pain on touch, no positive findings and mild redness of the vulva. There are very little minor glands in the vestibule that get inflamed and cause pain.
The vulvodynia can be classified into three categories : One is the intercourse despite being painful that can be carried out with some degree of discomfort. Second Category has to be discontinued due to pain and the Third is sex cannot happen.
Vulvodynia was primarily thought to be psycho sexual but we think that there is neural problems, these most often resolve in time.
Treat any existing problems that you may have come across during your investigation.
The explanation of the condition given to the patient and the reassurance that about seventy five percent can be treated helps them.
The general advice should emphasis is that they should not self medicate and get a clear cut diagnosis.
They can wash themselves with a freshly prepared saline solution consisting of two teaspoons of salt in a litre of water. They can use cold packs to relieve the pain, do not use commercial perfumes or antiseptics and wear light clothing. Try and improve your relationships and relieve the stress.
Follow the treatment for vaginismus , you may need help of a physiotherapist who is happy to give you bio feed back treatment. Electromagnetic treatment has been tried.
Neurological Antidepressants such as Amitriptyline with a small starting dose of 10mgs. It is thought to act as nerve membrane stabiliser.
Local lubricants (water based) are useful, oestrogen cream is useful in peri menopausal women.
Five percent Xylocaine cream can be applied at the time of intercourse.
Surgically vestibulectomy has been tried with significant improvement.
Now because we think that there is a neurological involvement we are doing more studies on the refining the diagnostic criteria and treatment of this very elusive condition.
The various other Vulvo Vaginal problems will be discussed in future posts.
Subscribe to:
Posts (Atom)